If you have burning, tearing, fluctuating vision; or if you’ve found benefit in warm eye compresses, the LipiFlow procedure can be of great benefit to you by improving symptoms and decreasing the need for medications, warm compresses or artificial tear drops. The procedure is completely safe and non-invasive and lasts twelve minutes. Plan on being at the office for at least thirty minutes total. Most people have no issue driving home after the procedure and it is not painful. If you are unsure if your symptoms are related to the oil layer of your tear film, a LipiView oil layer analysis can be administered to measure the thickness of your tear films oil layer. The procedure is not currently covered by any insurance carriers at this time, but you can use HSA or FSA. While this treatment is not ideal for everyone, there is nothing else available that can relieve oil layer deficient dry eye as well as LipiFlow. We will only have the LipiView and Lipiflow system in office every three months. The treatment will be available this upcoming Wednesday, September 6th and Thursday September 7th. To make an appointment, click the button below. If you have any further questions, please call the office and ask to speak to Dr. Biondo directly. 
3 Comments
 How would you describe the way you see the world without your glasses or contact lenses? While we would hope a child in school would be brave enough to say they can’t see the board at the front of the room, that can be difficult to admit for a young student. Also, they may not even be able to identify that their vision is poor. One in four children have a vision problem that can interfere with learning. A child needs many abilities to succeed in their studies and good vision is a key component. Reading, writing, chalkboard work and using computers are just a few of the visual tasks students perform daily. A child's eyes are constantly put to use in the classroom. When his or her vision is not functioning properly, education and participation can suffer. 60% of students identified as problem learners have undetected vision problems. All parents, we want to see our children do well in school and do all we can to provide them with the best educational opportunities. A child may not tell you that he or she has a vision problem because they may think that the way they see is the way that everyone sees. Signs that may indicate a child has difficulty seeing include:
80% of everything children learn comes from what they see. Most students are visual learners and in order to allow them to excel in their studies, accurate vision is crucial. We invite you to watch and share this video so that parents, guardians and teachers in order to encourage the awareness of children's vision issues. Ensure your child is seeing the blackboard clearly by making an appointment with Dr. Biondo today. Our main specialty at Kirkwood Eye Associates is the treatment and management of Keratoconus. We offer the latest in visual correction through our scleral lens prosthetic devices that offer patients with this condition the ability to see clearly with all day comfort and consistency. Until now, keratoconus management revolved around offering the best possible vision combined with careful monitoring of the progression. What was lacking was the ability to treat the condition itself, as keratoconus is a progressive disease that can result in the need for full corneal transplantation. Recently, the FDA approved a procedure known as corneal collagen cross-linking (C3R or CXL). This procedure, performed for over a decade in other developed countries around the world, is a safe and non-invasive treatment that aims to stop the progression of the disease in its tracks. CXL involves applying riboflavin (vitamin B2) to the cornea and exposing it to ultra violet light A (UVA), resulting in a reaction that strengthens the corneal tissue thereby stoping the progression of thinning and protrusion seen in keratoconus and post-LASIK ectasia. The procedure lasts 30-60 minutes and has a relatively fast recovery time. While it does not correct the corneal shape, it does stop it from getting worse and therefore preserves best-corrected visual acuity and greatly reduces the risk of corneal transplantation. The procedure is very safe and well tolerated and it is recommended for most any keratoconus patient under the age of 45, and a patient at any age who has post-LASIK ectasia. Because the cornea naturally cross-links with age, patients over 45 who show stable topography may not need CXL. The UVA light is absorbed by the cornea and the riboflavin. This is important because it can be harmful to the posterior cell layer of the cornea (the endothelium) if it is able to penetrate that far. For this reason, patients with corneas that have become excessively thin may not be good candidates for the procedure, although drops can be added prior to treatment to temporarily swell the cornea to a safe thickness. CXL does not cure keratoconus and those who are dependent on visual correction devices such as gas permeable lenses, hybrid lenses or scleral lenses will most likely continue to need these after the procedure is completed. Still, the stabilization will help to ensure that functional vision will always be possible and that the risk of corneal transplant is greatly diminished. To see if you would benefit from this new and exciting treatment option, contact Dr. Andrew Biondo and the team at Kirkwood Eye Associates for evaluation today. Combined with the revolutionary scleral lens systems for visual rehabilitation, normal visual function is more obtainable than ever before for patients with keratoconus and post-LASIK ectasia.  We recommend wearing sunglasses year round to protect your eyes from the sun's harmful UV rays, and you may be wondering what type to wear. Polarized lenses offer many advantages over their non-polarized counterparts and we highly recommend them as these lenses provide improved safety and vision. Polarized lenses were made popular by fishermen and boaters who needed something to protect them from the glare off the water. Polarized lenses block light rays that would normally enter your eyes after reflecting off of surfaces, such as a body of water or a shiny surface. The light that enters your eye after passing through a polarized lens has been filtered, offering the best visual quality and UV protection. 1. Reduced Glare On a sunny day, you may notice that objects on the horizon appear hazy, or that the light reflecting off your dashboard is nearly blinding. A polarized lens removes the effects of glare by blocking reflections off of other surfaces. This improves comfort and provides relief as you take in views without squinting. Roadways and water create major glare and create dangerous situations for drivers who may already struggle with their vision. Glare can create uncomfortable eye health issues for those with sensitive eyes, and may even cause migraines in patients who are prone to them. 2. Increases Visual Clarity Wearing polarized lenses reveals colors and images like never before. You will see crisply and cleanly, noticing intense detail that may surprise you. Squinting to see images stresses the eyes and creates uncomfortable eye health issues like redness, irritation, fatigue, and headaches. Polarized lenses neutralize this issue and allow eyes to feel more comfortable and well rested. 3. Enhanced Contrast Polarized lenses eliminate the harsh glare from the sun and help enhance colors and contrast leaving a remarkably crisp field of vision. Not only do polarized lenses reduce eye strain and make for safer driving and boating, they improve and enhance your perception of colors. Polarization can provide extremely crisp images with dazzling colors, which is why it is often used in photography. 4. Reduce Eye Strain Polarized lenses also reduce eyestrain. Most of us squint when we experience glare; when glare is gone there is often no need to stress your eyes to see clearly. So, if you drive a lot or spend a lot of time on or near water, consider polarized lenses that will help reduce the impact of a glare. Polarized lenses are the best option when glare is an issue because they absorb light from scattered angles. Enjoy your surroundings and spend more time doing the outdoor activities you love.. Non-polarized sun lenses filter all light whether it is ambient or reflected. By doing so, glare is diminished, but not eliminated. Colors may vary and details are not as crisp. People wear sunglasses for different reasons. Whether you sport your shades as a fashion statement, for comfort, or for your eye health, consider polarized lenses the next time you are purchasing sunglasses. 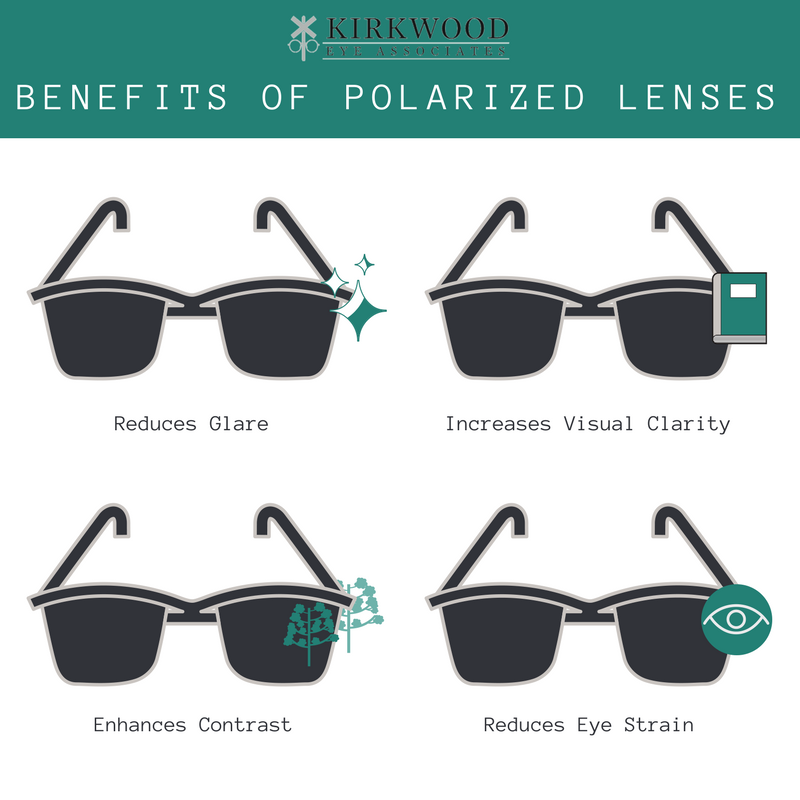 It is estimated that 41% of the population in the United States is myopic, or near-sighted. This is a 66% increase from just 30 years ago, and the incidence continues to rise. This is problematic for both financial and health reasons. The cost of vision correction, especially in those more highly myopic is becoming increasingly expensive. More importantly, individuals who are more myopic have a higher risk of glaucoma, early cataract, retinal detachment and some forms of macular degeneration, regardless of whether or not they correct their myopia with LASIK or some other vision correction surgery. There are many theories as to why we are becoming increasingly near-sighted. Most parents point to the increased use of electronic devices and overall increase in near-work. But there is no evidence to support that. The most recognized theories have proposed that we are becoming more near-sighted because we are spending more time indoors and not getting outside enough. Our eyes, as they develop, aren't exposed to long distances and therefore continue to elongate making us more near-sighted. The receptors in the eye responsible for this growth regulation are located in the periphery of the eye. Based on this theory, a child would be fine to sit and read a book all day, as long as they sat outside to do it. We typically develop near-sightedness during our school ages and this is the time that we can do something to slow or stop the progression. There are three options currently available that have shown an impressive ability to halt the worsening of myopia in children. ORTHOKERATOLOGY (Ortho-K) The first and arguably most effective is orthokeratology, or ortho k. This is a system that utilizes an overnight contact lens device to gently shape the cornea to remove near-sightedness and allow the child to see all day without the need for contacts or glasses. It is safe and easily reversible (simply discontinue the overnight use of the device). Some studies have shown a 100% decrease in the progression of myopia and this treatment is FDA approved for children of all ages. This is the best option because it eliminates the need for daytime glasses or contacts and has the best data to show that it stabilizes myopia MULTIFOCAL SOFT CONTACT LENSES The second tool in slowing the progression of myopia is the use of multifocal contact lenses. It is believed that the signal to grow the eye longer, and therefore make it more near-sighted, is triggered by your peripheral vision. As we spend more time indoors, our peripheral vision is exposed to more closed rooms and short distances as opposed to the infinite sight lines of being outside. Wearing certain types of multifocal soft contacts can trick your peripheral vision into thinking its outside while allowing the central vision to function normally. DROP THERAPY WITH ATROPINE Atropine drops have proven very effective in slowing or even stopping the progression of myopia in children and teenagers. This sounds like a perfect solution if not for the side effects seen with atropine use. This medication causes strong dilation of the pupil, making the child light sensitive and subject to glare at night. Atropine also inhibits the eyes ability to focus, making reading and near-work almost impossible. There are studies underway that are examining lower concentrations of atropine that those readily available to see if the side effects can be reduced or eliminated without losing the myopia control effects. What is myopia? Click the video below for more information.  Eyelid mites, know as Demodex, are believed to inhabit the eyelids and lashes of over 40% of the people in the United States. Theses mites, which live around two weeks and like to come out to eat and breed while we sleep, can cause ocular symptoms that are often mis-diagnosed as dry eye or ocular allergy. Demodex mites like to feed on the oily secretions of our hair follicles and oil glands, making the eyelids an ideal environment. They mites will burrow into the eyelash follicles and the meibomian glands that produce the oily layer of our tear film. For many people, there are no symptoms and the body’s natural defenses keep the mites in check. For others the infestation can lead to itching and burning eyes, redness and irritation, blurred vision and eyelid inflammation. It’s surprisingly easy to contract a demodex infection, which may explain why so many people have them crawling along their lids and lashes. Direct contact with infected skin is one means of contracting the mite, but some have been found to travel on dust, making it hard to avoid. There is also theories that pets may act as transmitters between hosts. Demodex infections can be easily diagnosed during an eye exam with a slit-lamp biomicroscope. The slit-lamps used in the exam rooms aren't powerful enough to view the mites directly, but an infection will show a very specific cylindrical dandruff pattern on the base of the lashes that is diagnostic for demodex mites. Demodex is also well documented to cause skin conditions, especially on the face including acne, rosacea and dermatitis. Eliminating the mites can prove tricky because they are not susceptible to many sterilization techniques. They also avoid daylight so they stay hidden within hair follicles and glands during the day and wait to emerge as we sleep to reproduce. Luckily, tea tree oil has proven effective at removing the infestation. It should be noted that tea tree oil is toxic to humans as well as the mites so it is not recommended to apply standard tea tree oil to the face and especially the eyes. Kirkwood Eye Associates offers tea tree foams that have been specially formulated for ocular use and can be used as complete face wash to clear signs of rosacea and acne as well. The foams are to be used twice daily and most importantly just before bed when the mites are known to come out. Kirkwood Eye Associates also recommends an initial in office treatment with concentrated tea tree and cleansing to achieve maximum results. If you experience irritation in or around the eyes, there is a good chance that the demodex mite is to blame. Call 314-394-3045 and set up an appointment today for an evaluation and treatment plan. LASIK has offered a safe and reliable method for correcting near-sightedness, far-sightedness and astigmatism. But what about those individuals over 45 years old that need help reading when they've been corrected for distance? Until now, there were three choices for patients who wanted corrective surgery over 45 years old. One was mono-vision LASIK, where one eye was corrected for distance vision and the other eye was corrected for near. This allowed for focusing up close and far away but it sacrificed binocularity (the two eyes working together) which often lead to compromised night vision and depth perception. The second option was reading glasses. This was hardly ideal considering the financial investment in a LASIK procedure that was supposed to eliminate the need for glasses. The final option was clear lens exchange (CLE) with a multifocal implant. This was essentially cataract surgery before a cataract was present. The implant could be equipped with multifocal optics to allow a range of vision and worked reasonably well, but it is expensive and invasive. We now have a new alternative for people wanting a minimally invasive vision correction surgery that allows for great distance and near vision without sacrificing binocularity. Corneal inlays have gained recent FDA approval and offer a safe and effective solution with a quick recovery time. Many patients who have surgery can return to work within two days. There are two types of corneal inlays available currently, the Raindrop inlay and the Karma inlay. These can be placed in just one eye and offer clear and comfortable intermediate (computer) and near vision, while allowing both eyes to continue to work together to optimize distance vision. The inlays can be placed under a LASIK flap if distance vision correction is required. If the patients distance vision is already optimal, the inlay can simply be placed in a grove in the front of the cornea. in addition, the inlay can be removed at any point. Corneal inlays have given patients over 45 years old a new and effective option in vision correction that LASIK had been previously unable to offer. If you have any questions about these new procedures or would like to see if you're a candidate, contact our office today and set up an evaluation.  Dry Eye affects people of all ages, but more women than men are affected. Causes can include genetics, hormonal changes, prescription medications and systemic diseases like diabetes or autoimmune conditions. Symptoms of dry eye disease range widely from the occasional use of artificial tears to the inability to function in everyday life. The disease typically worsens as we get older so seeking treatment earlier can prevent the need for more aggressive treatments down the road. So what can we do about it? Luckily, a flood of new and effective treatment options have been released over the past two decades that have allowed for the relief of dry eye symptoms. Artificial tears and topical lubricants can offer temporary relief but are only palliative and do not actually treat the underlying cause of the disease. The first step in selecting the proper treatment is to understand the cause of the dry eye. Some cases are caused by an inability to produce tears (aqueous deficient dry eye) and others lack the crucial oil layer of the tear film that protects the tears from evaporation (evaporative dry eye). Simple examination and testing can help to determine which type of dry eye is causing symptoms. To treat aqueous deficient dry eye we focus on reducing the inflammation that causes the tear glands to not function properly. Prescription medications like Restates and Xiidra help to reduce the inflammation on the surface of the eye, relieving the discomfort and allowing the tear glands to work normally. For some people, more severe treatments are needed including topical corticosteroids or amniotic membrane treatments. Once inflammation is under control, punctual plugs, a safe, easy and painless procedure done in office, can act to slow the drainage of tears off the surface of the eye, allowing more natural tear to remain for longer periods of time. For those with evaporative dry eye, treatments tend to focus on the eyelids. Oil glands located in the lids secreted oil onto the surface of the eye to prevent the evaporation of tears between blinks. If these glands become blocked or the oil becomes unhealthy, the tears will not protect the ocular surface properly. Treatment typically begins with warm compresses, foaming lid cleansers and oral supplements to improve the function of the oil glands and remove any blockages. If this is not sufficient, oral pharmaceuticals may be needed along with in office procedures to clear out the glands such as the Lipiflow Thermal Pulsation System. These two types of dry eye are not mutually exclusive and many patients may need both types of treatments. Over-the-counter drops will only offer short term relief and will not stop the progression of the disease. While we cannot cure dry eye disease, we now have the tools to treat it effectively in a way that allows patients to live pain free and without fluctuating vision and/or irritation throughout the day. 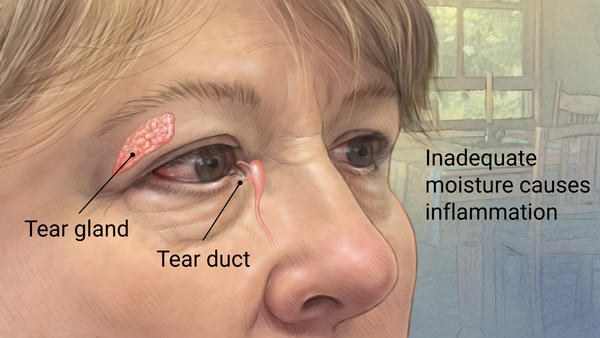 Image courtesy of Mayo Clinic and Google Images.
LED screens are ingrained in our society. My nieces learned to use an iPhone and iPad before they could walk. Smartphones, tablets, computer monitors, touch-screens; They are everywhere and used by almost everyone. While there's no denying their importance and benefits, the question that we’re still trying to answer is what are they doing to our eyes? Recent research shows higher than normal percentages of blue-violet wavelengths being emitted from these devices. The blue-violet spectrum is in the visible light spectrum adjacent to the UV light portion of the spectrum (see figure below). 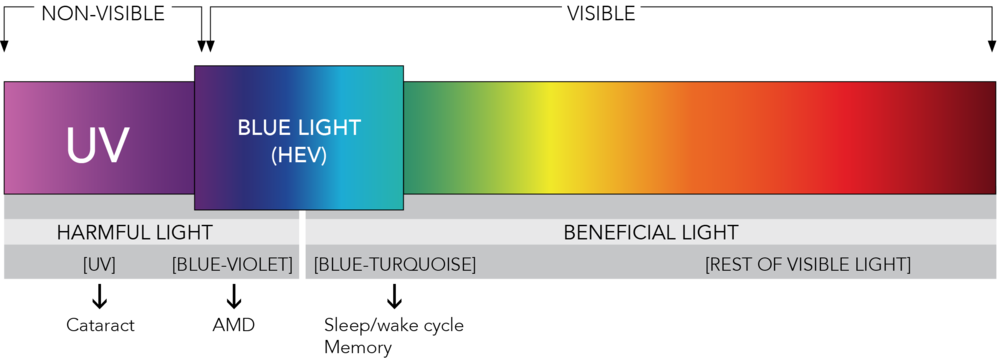 UV light and its detrimental effects are well known and well documented. UV light is made of shorter wavelengths that the visible light our eyes can process and shorter wavelengths carry higher energy. This high energy form of light can damage our cells and the DNA within, allowing UV light to damage our skin and potentially cause cancer.
While there is no evidence that blue-violet light causes cancer, recent studies have shown that it does cause damage to retinal cells. With this data it is theorized that higher quantities of blue-violet light could raise ones chances of developing retinal diseases including macular degeneration. Our eyes have natural defenses that keep UV light from reaching the retina, but blue-violet light is in the visible spectrum and is therefore allowed to pass through to the retinal unchecked. The higher percentages of this high-energy light given off my LED devices may be doing more harm than we know. Pediatricians are already warning parents to not allow their babies to use tablets and smart phones in order to protect them from the harmful effects on the retina. If you move a little further up the spectrum from UV, you get to the blue-turquoise light that our brain uses to regulate our sleep/wake cycle. This light is also given off in higher percentages from LED devices and this can lead to poor sleep patterns and difficulty falling asleep. Luckily, there are ways to protect your eyes and properly regulate the blue violet and blue turquoise light that reaches your retina. New coatings placed on prescription glasses can block percentages of blue-violet light from reaching the eye, allowing only the natural amount through for proper color perception. Two such coatings, Crizal Prevencia and Hoya Recharge are already available at many eye doctors offices. These coating serve many purposes including glare reduction, scratch protection, UV protection, smudge reduction and, most importantly, blue-violet light filtration. What if you don’t already wear glasses? With all of the computer and tablet use being seen today in the workplace, our focusing systems are more stressed than ever and this results in eye fatigue, headache and worse. New anti-fatigue lenses are gaining popularity for people who don’t typically need an eyeglass prescription to see at any distance. These lenses aid your focusing system and take stress off of the eye while working and still allow clear distance vision for driving and other activities. The blue-violet coatings can then be applied to these lenses to offer protection to go along with the anti-fatigue properties. These anti-fatigue lenses with the anti-blue violet coatings are also great to use over contact lenses, or can be made with your prescription if you have near-sightedness, far-sightedness or astigmatism. Call Kirkwood Eye Associates today to see what option would work best for you, even if you're seeing well and don’t need glasses or contact lenses. For the past four decades, we’ve basically had two choices when it came to contact lenses. The first choice was the ‘hard lens’ (eventually replaced by the gas permeable, or GP lens). Hard lenses and GP’s offer the best vision of any contact lens because the rigid material allows for the crispest optics. The rigidity also helps fill in (with the help of your tears) any imperfections on the corneal surface and therefore automatically accounts for astigmatism and irregularity, allowing for improved vision. The downside of hard lenses is the comfort. It can take up to six weeks to adapt to the comfort of wearing a GP lens all day. Symptoms early on can include excessive blinking, eye watering, foreign body sensation and even pain. For certain people with eye conditions that affect the cornea (keratoconus, corneal transplant, corneal trauma, etc.), hard lenses are a necessity because they smooth out the irregular surface and allow for much better vision than glasses or soft contacts. To combat the comfort issue, the soft contact lens was introduced and has since dominated the market. These were often comfortable from the moment you first wore them and offered serviceable vision. Because they're not hard, the optics are not as crisp as those of a GP lens, and any astigmatism must be corrected because it is not masked like it is with a GP lens. Most people find the mild compromise to their vision acceptable given the comfort and short adaptation time to soft lenses. Soft lenses can also cause issues with dryness when the lens become dehydrated, and allergens can more easily adhere to a soft lens, making them often troublesome to allergy sufferers. While the hard lens can offer better vision, convenience is king in today’s world and soft lenses are here to stay. A new type contact lens called a scleral lens is hoping to take the compromise out of contact lenses. It’s made from a gas permeable material, giving the improved optics seen with the older style of GP’s, but it fits on the sclera (the white part of the eye) and vaults over the cornea, offering greatly improved comfort that is often comparable to a soft contact lens. This allows for sort of ‘win-win’ scenario in which the wearer gets GP quality vision with soft lens quality comfort. These lenses are especially helpful for people with corneal diseases like keratoconus, but the vision-to-comfort ratio makes them a great choice for anyone who wears contacts or is interested in contacts. Because they are made from a gas permeable material, they cannot dry out and are a terrific option for people who suffer from contact lens dryness or dry eye disease. In fact, scleral lenses can be used therapeutically to treat people with dry eye syndrome. Newer multifocal designs have shown great distance and near vision for wearers over forty who need reading glasses or bifocals to read. Scleral lenses are custom made to fit your eyes and your vision. They require a diagnostic in-office fitting to size and power the lens just for you. Because they are a custom device, there is no longer any sacrifice for people who had prescriptions outside of the ‘normal’ ranges. Give us a call today if you live in or around the St. Louis area and let us find out if you would make a good scleral lens candidate. |

AuthorAndrew Biondo, OD, FSLS is the Primary Medical Director at Kirkwood Eye Associates in Kirkwood, MO. Serving the greater St. Louis area, Dr. Biondo has 12 years of experience as an eye care provider, health educator & consultant to the specialty contact lens industry. His special interests include contact lenses, dry eye disease, glaucoma, macular degeneration, laser eye surgery & preventive vision care. Archives
October 2022
Categories |
 RSS Feed
RSS Feed
Contact us:
|
Location:
|
Stay in the loop!
|